Daily routine:
He is a farmer by occupation.
Resident of Miryalagudem
Stopped working 2 years ago due to right femur fracture and old age.
Wakes up at around 7:00 am in the morning. Eats breakfast by 8:00 am. Goes to his farm and monitors work. Then comes back to his house in the afternoon and has lunch by 1:00 pm. Sleeps for a while in the afternoon
He has a cup of tea in the evening at around 5:00 pm , watches TV for a while and has dinner at around 8:00 pm and goes to bed at around 9:30 pm.
Chief complaints:
Patient was brought to casualty with c/o shortness of breath Grade III MMRC since 20 days
HOPI
Patient was apparently asymptomatic 1 year ago when he developed angina and SOB Grade III and went to a hospital in Hyderabad
where he was diagnosed with CAD-evolved IWMI MOD LV DYSFUNCTIONLRTI BASAL ATELECTASIS
Coronary Angiogram was done through radial route on 15/11/22-
PTCA-STENTING TO MID LAD WITH 2.5X28MM(ALPINE) DONE ON
LMCA-NORMAL
LAD-TYPE III VESSEL, MID tandem lesions with 75% STENOSIS DIAGONAL-NORMAL
LCX-NON DOMINANT, proximal 80% stenosis
OBTUSE MARGINAL-diffuse disease distally RCA DOMINANT, proximal focal 90% stenosis, distal normal
PDA-NORMAL
PICA STENTING TO PROX-MID RCA WITH 3.0X42MM BIOFREEDOM
PLV-DIFFUSE DISEASE
2D ECHO ON 15/12/23
On 26/6/23 -
Patient was taken to hospital in Miryalagudem as he had SOB and sweating and diagnosed with ? Pulmonary edema
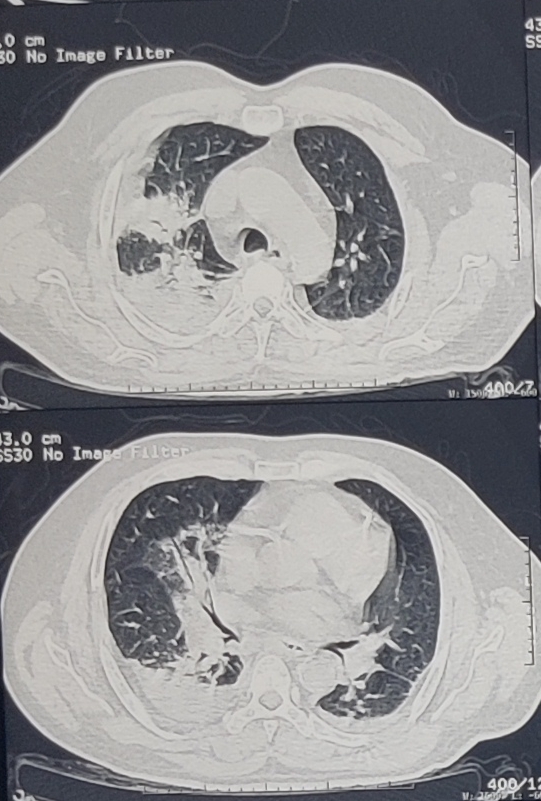
HRCT REPORT THORAX:
CT PULMONARY ANGIOGRAM -
There the patient was advised for admission and was there in the hospital for a week and was discharged
But patient has started to develop SOB Grade III again on 9/7/23 and hence was brought to our hospital
Presently- on 9/7/23
20 days back he developed Shortness of breath Insidious in onset , initially Grade I and gradually progressed to Grade-III.
It was associated with Right sided chest pain , non radiating , pricking type of pain
It was also associated with PND, dry cough and sweating
No c/o orthopnea, palpitations and giddiness
Patient also C/o B/L lower limbs swelling since 5-6 months, pitting type, extending upto the knee, aggravated on sitting, standing and walking and relieved on lying down.
Patient also complains of decreased urine output and facial puffiness since 3 days
He also complains of constipation- passes stools every 3-4 days.
He also has distended abdomen since 3 days
No c/o pain abdomen, vomitings, fever, cough, cold.
PAST HISTORY -
Patient is k/c/o DM 2 since 5 years and is on regular medication - Tab. Metformin 500 mg BD
He is also a k/c/o Hypertension since 5 years and is on regular medication - Tab. Metoprolol 25 mg + Tab. Amlodipine 5mg OD
H/o CAD 1 year ago - underwent Percutaneous Transluminal Coronary Angioplasty with 3 stents- done along with Tab. Atorvas 10mg + Tab. Clopidogrel 75 mg.
Not a k/c/o TB, Asthma, Epilepsy, Thyroid disorders and CVA.
H/o Right femur fracture 2 years years ago, underwent open reduction and internal fixation.
Underwent Knee replacement for Left knee 7 years ago.
PERSONAL HISTORY:
Diet: Mixed
Appetite: Normal
Sleep: Adequate
Bladder: Decreased urine output.
Bowel : Constipation+ (Passes stools once in 3-4 days )
Patient was an alcoholic and cigarette smoker for about 15 years.
Stopped alcohol 10 years ago.
Stopped smoking 20 years ago.
No known allergies
FAMILY HISTORY:
No significant family history
GENERAL EXAMINATION:
Patient is conscious, coherent and cooperative
Patient was examined in well lit room after taking well informed consent.
Patient is moderately built and moderately nourished.
Pitting edema Grade III present.
No pallor/icterus/cyanosis/clubbing/Generalized lymphadenopathy
VITALS ON ADMISSION -
Temp: Afebrile
PR: 88 bpm
RR: 17 cpm
BP: 130/80mmHg
Spo2: 87% @RA
GRBS: 202 mg/dl
SYSTEMIC EXAMINATION:
CVS: S1 S2 heard, No murmurs
RS: BAE+, crepitations + in Left IAA
P/A: Distended, non tender
Umbilicus - Central
No engorged veins, scars or sinuses
1. Autonomic function: Normal
2. CNS examination:
Pupils -B/L NSRL
GCS - E4V5M6
Cranial nerves - NAD
MOTOR SYSTEM :
Rt Left
Bulk: N. N
Tone: Rt Left
UL. N N
LL. N N
Deep tendon reflexes:
Biceps: +2 +2
Triceps: +2 +2
Supinator: +1 +1
Knee: +2. +2
Ankle: +2 +2
Plantar: flexor B/L
Sensory system : Intact
PROVISIONAL DIAGNOSIS -
?Heart failure ?COPD
INVESTIGATIONS on 9/7/23-
ECG-
USG abdomen -

Chest X-Ray:PA view
CTPA (26/6/23)
Hemogram -
Hb: 9.6 gm/dl
TLC: 8,100
N/L/E/M/B - 75/15/ 1/10/0
RBC - 3.77
Platelets :3.30
PBS:NC/NC
RBS - 148 mg/dl
Urea: 41 mg/dl
Creatinine: 1.2
Na: 143
K: 4.3
Cl: 98
Ca (ionized)- 1.12
Total bilirubin - 1.39
Direct bilirubin - 0.29
AST- 27
ALT - 24
ALP - 141
Total protein - 5.8
Albumin 3.16
A/G: 1.20
CUE: Albumin +
Sugar- ++++
Ep cells - 5-6
Pus cells -2-4
HBsAG - negative
HCV- negative
HIV 1/2 -negative
TREATMENT:
1) INJ. LASIX 50 MP IV/BD
2) TAB. METFORMIN 500MG PO/BD
3) TAB. AMLONG MT 5/25 MG PO/OD
4) TAB. ATOCOR CV 10 PO/ OD
5) TAB. PULMOCLEAR 100/600MG PO/BD
6) SYP. ASCORIL D 10ML PO/TID
7) NIV
8) LASIX INFUSION AT 5ML / HOUR
9) TAB RAMIPRIL 2.5 MG PO/OD
10/07/2023
S:
2 fever spikes at 4 and 6 am
SOB and cough decreased
O:
Patient is conscious coherent and cooperative
No icterus,cyanosis,clubbing,
lymphadenopathy
Bp-120/80mmHg
Pr- 92 bpm
Temperature - Afebrile
Rr- 19 cpm
Spo2- 92% on RA
Grbs- 149mg/dl @8am
I/o-240/2600 ml
CVS-S1,S2 heard ,no murmurs
RS- BAE present
NVBS ,Mild crepts in Left IAA
CNS-
Pupils- B/L NSRL
GCS - E4V4M6
Deep tendon reflexes:
Biceps: +2 +2
Triceps: +2 +2
Supinator:. + +
Knee: +2 +2
Ankle: +2 +2
Plantar: flexor flexor
P/A- Soft, NT
A:
SOB UNDER EVALUATION
?HEART FAILURE
?COPD
K/C/O HTN AND DM II SINCE 6 YEARS
S/P : PTCA 1 YEAR AGO
P:
1. Intermittent NIV
2. Inj. Lasix infusion @2.5ml per hour
3. Tab. Metformin 500 mg PO/BD
4. Tab. Amlodipine 5 mg + Metoprolol 25 mg PO/OD
5. Tab. Atorvas - CV PO/OD
6. Tab. Ramipril 2.5 mg PO/OD
7. Tab. Pulmoclear 100/600 mg PO/BD
8. Tab. Ascoryl 10 ml PO/ TID
Investigations:
FBS - 147 mg/dl
PLBS - 248 mg/dl
HbA1c- 7.1
Hemogram:
Hb: 9.6 gm/dl
TLC: 6, 700
N/L/E/M/B - 70/16/ 1/10/0
RBC - 3.67
Platelets : 2.89
PBS:NC/NC
Serum electrolytes-
Na: 142
K: 3.6
Cl: 98
Ca (ionized)- 1.00
11/07/2023
S:
2 low grade fever spikes
SOB decreased
O:
Patient is conscious coherent and cooperative
No icterus,cyanosis,clubbing,
lymphadenopathy
Bp-130/80mmHg
Pr- 86 bpm
Temperature - Afebrile
Rr- 22 cpm
Spo2- 85% on RA and 94% on 2 litres of O2
Grbs- 171 mg/dl @8am
I/o-700/1700 ml
CVS-S1,S2 heard ,no murmurs
RS- BAE present
NVBS ,Mild crepts in Left IAA
CNS- NFAD
P/A- Soft, NT
A:
HEART FAILURE WITH MIDRANGE EJECTION FRACTION (EF - 45%)
?COPD
K/C/O HTN AND DM II SINCE 6 YEARS
S/P : PTCA 1 YEAR AGO
P:
1. Intermittent NIV
2. Inj. Lasix 40 mg IV/BD @2.5ml per hour
3. INJ.HAI S/c TID premeal according to GRBS
4. Tab. Amlodipine 5 mg + Metoprolol 25 mg PO/OD
5. Tab. Atorvas - CV 10/75 PO/HS
6. Tab. Ramipril 2.5 mg PO/OD
7. Tab. Ascoryl 10 ml PO/ TID
8. Syrup. Cremaffin plus 15 ml PO/ HS
Investigations:
Hemogram:
Hb: 9.4 gm/dl
TLC: 5500
N/L/E/M/B - 70/25/3/2/0
RBC - 3.60
Platelets : 2.50
PBS:NC/NC
Serum electrolytes-
Na: 138
K: 3.5
Cl: 99
Ca (ionized)- 1.19
ECG -
Chest x-ray
12/07/2023
S:
3 low grade fever spikes
SOB decreased
O:
Patient is conscious coherent and cooperative
No icterus,cyanosis,clubbing,
lymphadenopathy
Bp-110/80mmHg
Pr- 98 bpm
Temperature - 98.8F
Rr- 20 cpm
Spo2- 88% on RA and 98% on 4 litres of O2
Grbs- 245 mg/dl @8am
I/o-1300/2000 ml
CVS-S1,S2 heard ,no murmurs
RS- BAE present
NVBS , no added sounds.
P/A- Soft, NT
A:
HEART FAILURE WITH MIDRANGE EJECTION FRACTION (EF - 45%)
?COPD
K/C/O HTN AND DM II SINCE 6 YEARS
S/P : PTCA 1 YEAR AGO
P:
1. Intermittent NIV
2. Inj. Lasix 40 mg IV/BD @2.5ml per hour
3. INJ.HAI S/c TID premeal according to GRBS
4. Tab. Amlodipine 5 mg + Metoprolol 25 mg PO/OD
5. Tab. Atorvas - CV 10/75 PO/HS
6. Tab. Ramipril 2.5 mg PO/OD
7. Tab. Ascoryl 10 ml PO/ TID
8. Syrup. Cremaffin plus 15 ml PO/ HS
13/07/2023
S:
No fever spikes
SOB decreased
O:
Patient is conscious coherent and cooperative
No icterus,cyanosis,clubbing,
lymphadenopathy
Bp-120/80mmHg
Pr- 86 bpm
Temperature - 98.7F
Rr- 20 cpm
Spo2- 98% on RA
Grbs- 253 mg/dl @8am
I/o-1000/1700 ml
CVS-S1,S2 heard ,no murmurs
RS- BAE present
NVBS , no added sounds.
P/A- Soft, NT
A:
HEART FAILURE WITH MIDRANGE EJECTION FRACTION (EF - 45%)
?COPD
K/C/O HTN AND DM II SINCE 6 YEARS
S/P : PTCA 1 YEAR AGO
P:
1. O2 support
2. Strict I/o , vitals charting and restrict mobility.
3. INJ.Human Mixtard 30/70 S/c BD 15 units
4. Tab. Metoprolol 25 mg PO/OD
5. Tab. Atorvas - CV 10/75 PO/HS
6. Tab. Ramipril 2.5 mg PO/OD
7. Tab. Ascoryl 10 ml PO/ TID
8. Syrup. Cremaffin plus 15 ml PO/ HS
Investigations:
Hemogram:
Hb: 9.8 gm/dl
TLC: 4600
N/L/E/M/B - 70/21/3/6/0
RBC - 3.72
Platelets : 1.89
PBS:NC/NC
Serum electrolytes-
Na: 139
K: 3.6
Cl: 101
Ca (ionized)- 1.11
Chest x ray - PA view 13/7/23
14/07/2023
S:
No fever spikes
Yesterday night he had SOB and today SOB reduced.
O:
Patient is conscious coherent and cooperative
No icterus,cyanosis,clubbing,
lymphadenopathy
Bp-160/70mmHg
Pr- 94 bpm
Temperature - 96.5F
Rr- 20 cpm
Spo2- 90% on RA
Grbs- 296mg/dl @8am
I/o-1250/2750ml
CVS-S1,S2 heard ,no murmurs
RS- BAE present
NVBS , no added sounds.
P/A- Soft, NT
A:
HEART FAILURE WITH MIDRANGE EJECTION FRACTION (EF - 45%)
?COPD
K/C/O HTN AND DM II SINCE 6 YEARS
S/P : PTCA 1 YEAR AGO
P:
1. O2 support
2. Strict I/o , vitals charting and restrict mobility.
3. INJ.Human Mixtard 30/70 S/c BD 15 units
4. Tab. Metoprolol 25 mg PO/OD
5. Tab. Atorvas - CV 10/75 PO/HS
6. Tab. Ramipril 2.5 mg PO/OD
7. Tab. Ascoryl 10 ml PO/ TID
8. Syrup. Cremaffin plus 15 ml PO/ HS
9.Fluid restriction
10.Strict I/O charting
11.Oxygen support to maintain saturation
12.BP,PR,RR,SPO2 monitoring 2nd hourly.
15.7.23
S:
No fever spikes
Yesterday night he had SOB and today SOB reduced.
O:
Patient is conscious coherent and cooperative
No icterus,cyanosis,clubbing,
lymphadenopathy
Bp-150/100mmHg
Pr- 92 bpm
Temperature - 96.5F
Rr- 20 cpm
Spo2- 86% on RA, 96% on 1lit O2
Grbs- 171 mg/dl @8am
CVS-S1,S2 heard ,no murmurs
RS- BAE present
NVBS , no added sounds.
P/A- Soft, NT
A:
HEART FAILURE WITH MIDRANGE EJECTION FRACTION (EF - 45%)
?COPD
K/C/O HTN AND DM II SINCE 6 YEARS
S/P : PTCA 1 YEAR AGO
P:
1. O2 support
2. Strict I/o , vitals charting and restrict mobility.
3. Inj. HAI S/c TID and Inj. NP S/C BD
4. Tab. Metoprolol 25 mg PO/OD
5. Tab. Atorvas - CV 10/75 PO/HS
6. Tab. Ramipril 2.5 mg PO/OD
7. Tab. Ascoryl 10 ml PO/ TID
8. Syrup. Cremaffin plus 15 ml PO/ HS
9.Fluid restriction< 1 lit/day and salt restriction< 2g/ day
10.Strict I/O charting
11.Oxygen support to maintain saturation
12.BP,PR,RR,SPO2 monitoring 2nd hourly.
Hemogram:
Hb: 10.3 gm/dl
TLC: 6100
N/L/E/M/B - 87/25/3/5/0
PCV - 32.5
RBC - 3.08
Platelets : 1.61
PBS:NC/NC
Serum electrolytes-
Na: 144
K: 3.6
Cl: 101
Ca (ionized)- 1.11
Hb: 10.2 gm/dl
TLC: 7400
N/L/E/M/B - 59/33/3/5/0
PCV - 32.5
RBC - 3.87
Platelets : 1.77
PBS:NC/NC
17/07/2023
S:
No fever spikes
No SOB
O:
Patient is conscious coherent and cooperative
No icterus,cyanosis,clubbing,
lymphadenopathy
Bp-120/90mmHg
Pr- 91bpm
Temperature - 98F
Rr- 21 cpm
Spo2- 96% on RA
Grbs- 142 mg/dl @8am
I/o-900/1100ml
CVS-S1,S2 heard ,no murmurs
RS- BAE present
NVBS , no added sounds.
P/A- Soft, NT
A:
HEART FAILURE WITH MIDRANGE EJECTION FRACTION (EF - 45%)
? COPD
K/C/O HTN AND DM II SINCE 6 YEARS
S/P : PTCA 1 YEAR AGO
P:
1. Tab. METOPROLOL 25mg PO/OD
2. Tab. RAMIPRIL 2.5mg PO/OD
3. Tab.ATORVAS - CV (10/75) PO/HS
4.Tab. DYTOR 10mg PO/BD
6. Tab. AMLODIPINE 5mg PO/OD
7. INJ. HAI s/c TID before meals
INJ. NPH s/c BD before meals according to GRBS
8. Tab. Ascoryl 10 ml PO/ TID
9. Syrup. Cremaffin plus 15 ml PO/ HS
10. Fluid restriction <1.5L/day
Salt restriction <2g/day
11. Strict I/O charting
12. Vitals monitoring 4th hourly
BP monitoring 2nd hourly
13. O2 inhalation to maintain spO2 >92% increase/decreased according to saturation.
Patient was discharged on 17/7/23 with the following -
Advice at Discharge-
1.INJ. HAI TID
16U-16U-14U
INJ.NPH BD
14U-X-14U
2.TAB. METOPROLOL 25MG PO/OD
3.TAB RAMIPRIL 2.5MG PO/OD
4.TAB DYTOR 10MG PO/BD
5. TAB AMLODIPINE 5MG PO/OD
6.TAB.ATORVAS-CV (10/75) PO/HS
7.SYP. CREMAFFIN PLUS 15ML PO/HS
8. FLUID RESTRICTION <1.5L/DAY
SALT RESTRICTION<2G/DAY
Follow Up
PATIENT WAS ASKED TO REVIEW AFTER 10 DAYS TO MEDICAL OPD

































Comments
Post a Comment